|
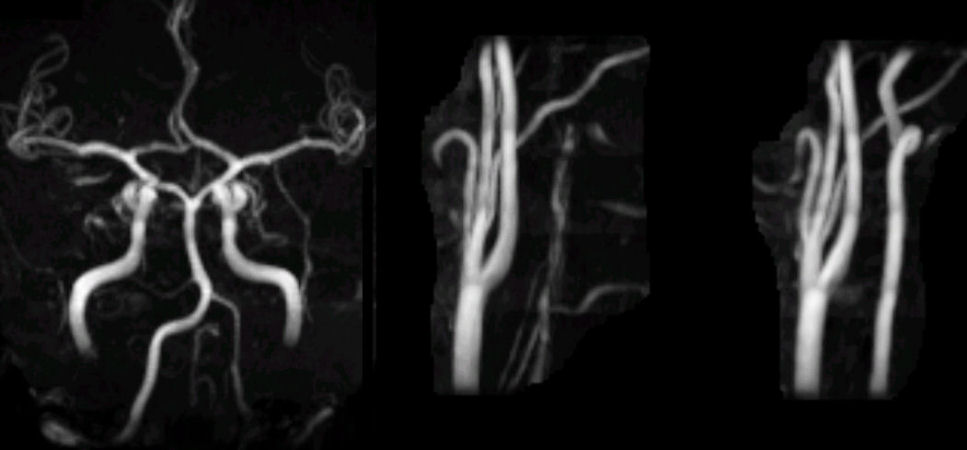
A 34 year-old man developed transient vertigo associated with left neck pain. |
![]()
| Vertebral Artery Dissection: Magnetic resonance angiogram; (Left)
intracranial; (Middle) left neck; (Right) right neck. Note the normal caliber of the
right vertebral and basilar arteries.
In contrast, the left vertebral artery is very small intracranially and poorly seen in the
neck. This picture could result from a congenital hypoplastic vertebral artery or from
a dissection and a subsequent "string sign." CCA = common
carotid artery; ICA = internal carotid artery; MCA = middle cerebral
artery; ACA = anterior cerebral artery. If the diagnosis of dissection is suspected, fat-suppression MRI is the imaging study of choice. Intramural blood can be well demonstrated on these scans. Routine magnetic resonance angiography (MRA) will often demonstrate narrowing or occlusion of the vessel, but in most cases cannot differentiate dissection from other etiologies. It is critical to detect a dissection before ischemia occurs, so that treatment can be promptly initiated. Arterial dissection occurs due to a tear in the intimal layer of the artery. The tear allows blood to enter the wall and form an intramural hematoma. Depending on which layer of the blood vessel is involved, either a subintimal or a subadventitial hematoma develops. A subintimal hematoma tends to cause stenosis of the artery, whereas a subadventitial hematoma often results in aneurysmal dilatation of the artery. In the case of stenosis, sluggish blood flow distal to the dissection results in the formation of fibrin clot. The clot continues to enlarge and eventually breaks off to travel and dislodge downstream as an embolus. Although rare in the general population, dissections of the carotid and vertebral arteries account for a substantial number of strokes in young adults and middle-aged patients. Most dissections involve some type of trauma or stretch to the head or neck. Sometimes, the trauma is trivial and forgotten by the patient. There is a higher incidence in certain congenital connective tissue disorders, including Marfan's syndrome, cystic medial necrosis, and fibromuscular dysplasia. The recognition of an arterial dissection requires a high degree of clinical suspicion and an ability to recognize some key neurological signs which help to key in on the diagnosis. The classic symptoms and signs of vertebral artery dissection
include the following: • Pain in the back of the neck,
although it can be diffuse or frontal |
Revised
11/29/06
Copyrighted 2006. David C Preston